
Unlocking reform and financial sustainability: NHS payment mechanisms for the integrated care age
Payment mechanisms for ICSs: What should the NHS be considering now, next and in future?
Looking to the future, the NHS in England will need to consider what form of payment mechanism could best support ICSs to meet their objectives set out above and remove the barriers to tackling the challenges described. This paper sets out three potential models for consideration. These models have been proposed following discussion with the Payment Mechanism Working Group and following engagement with some NHS Confederation members, experts and wider stakeholders, as well as reflections on existing types of payment mechanism and international case studies which are highlighted in the paper. The models are presented to contribute to further debate and experimentation but are not intended to represent an ideal type nor a specific view on behalf of NHS Confederation members.
The models have been proposed in response to the specific challenges facing the sector. Given the structural challenges and immediate pressures on the NHS, improving productivity is crucial. Each approach should also seek to minimise complexity and safeguard against risks and unintended consequences. While each has its strengths and weaknesses and may be better suited in certain contexts, overall they seek to advance the leftward/upstream shift towards more preventative health and allocative efficiency as well as helping to drive technical efficiency.
The three models are presented in order of timeliness – some will require more work to develop the appropriate detail and implement than others. Those which require further work represent a more significant shift from the status quo and are potentially better suited to ICSs but are not yet ready to implement. We therefore describe these as options for consideration ‘now’, ‘next’ and ‘in future’, based on how much further work would be required.
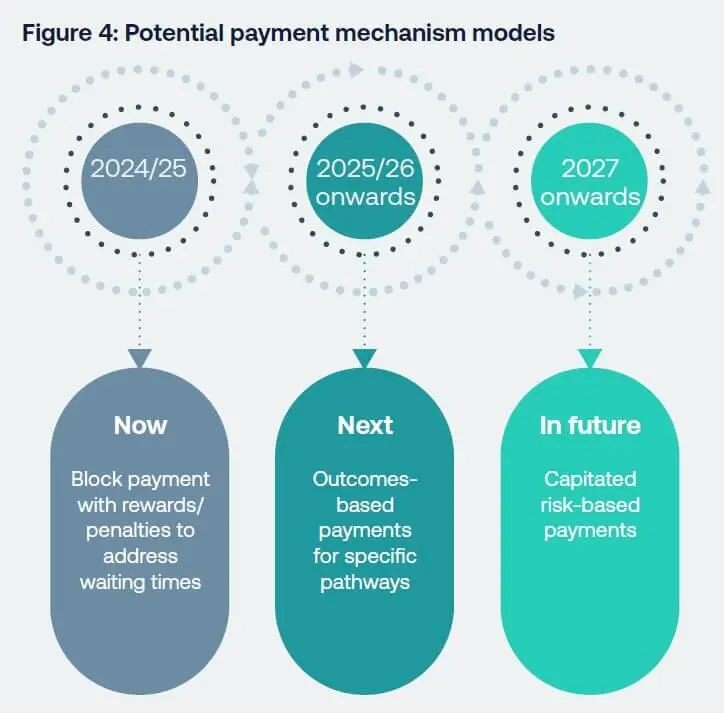
Figure 4 in plain text: Potential payment mechanism models
- 2024/25: Now - Block payment with rewards/ penalties to
address waiting times - 2025/26 onwards: Next - Outcomes-based payments for specific
pathways - 2027 onwards: In future - Capitated risk-based payments
Now: Block payment with rewards/ penalties to address waiting times
The current 2023-25 NHS Payment Scheme has another year to run at the time of publication (with some minor midway adjustments). In the immediate run up to and in the wake of the 2025 general election, increasing the volume of secondary elective activity to reduce waiting times and waiting lists for elective acute care is likely to remain a political priority. Additionally, the drive for greater technical productivity in acute services, where most NHS money is still spent, will likely be high on the agenda of the next government.
The political reality is that any dramatic move from both payment by activity or financial incentives for elective care is unlikely in the short term. We must still recognise that, while intended to reduce elective waits, the present payment scheme is a counter-vailing force against the ICS mission for a left-shift to more preventative care, as it incentivises generally more expensive secondary care activity and undermines allocative efficiency. Within this context, ICSs (both ICBs and provider partners) may seek to innovate using the flexibility within the current payment scheme, although there is no perfect ‘off the shelf’ model ready to be put into practice.
In the immediate term, local ICSs may want to consider adopting and/or adapting the ‘West Yorkshire’ model, subject to further evaluation (see case study page 25). This model includes a combination of block payment, enabling service change, and fee for service, to reduce waiting times across the provider collaborative. Waiting time targets are agreed between the commissioner and providers, who face a £2,000 penalty for every 52-week waiter above their target number at the end of March 2024. Conversely, trusts that beat their target will receive a £2,000 bonus per patient, and there are no caps for under or over-performance. This can help address long waits and the backlog of elective care without losing the benefits of collaboration and clinical innovation that a level of fixed income had enabled. It also provides a reward for higher value interventions that prevent people from become long waiters, although not necessarily across multiple care settings. In particular, the block payment element of the contract has also enabled innovation in service model delivery and greater productivity that was disincentivised under PbR arrangements.
We present this option as an attempt at a ‘quick fix’ to address the elective care waiting lists while curbing some of the disadvantages of payment by activity, without an evaluation having yet been conducted. However, to support the leftward/upstream shift towards more preventative care and to incentivise greater integration of services, we believe other options are more desirable in the longer term. We would propose ICS explore opportunities for local experimentation, including approaches such as the West Yorkshire model. Wider use of and learning locally agreed payment mechanisms should be encouraged nationally.
Next: Outcomes-based payments for specific pathways
Looking beyond short-term political priorities, to deliver on their first core purpose of improving population health and outcomes, ICSs should focus on improving and measuring improvements in specific health outcomes, not just output such as the volume of activity. Shifting focus to ends rather than means could enable greater innovation within systems, driving improvements in technical efficiency. Payments based on outcomes can incentivise both providers and payers to deploy early-stage and more cost-effective interventions, boosting allocative efficiency, provided there is an appropriate ‘gain-share’ mechanism to ensure all system partners see a financial benefit from this.
This model would involve introducing an outcome-based fee for specific therapy areas, paid in exchange for delivering against agreed specific outcomes for a specified population, rewardingand incentivising preventative interventions which align with care pathways. This would commission services around pathways, not providers, and stretch across primary, community and secondary care providers, encouraging them to work together towards shared goals and incentivising integration.
To ensure this approach provides a ‘gain-share’ to different providers, it may be beneficial for an ICB to commission a lead provider to sub-commission further interventions – either upstream preventative admissions, if an acute provider, or later secondary care, if a primary or community provider. This would replicate the savings incentive seen in the American ChenMed and German OptiMedis case studies (see above). However, negotiating payments between providers can be a long and cumbersome process.
Learning from QOF (see payments for quality/outcome, above) this model should therefore focus on measurement and payment for a small number of defined and agreed patient outcomes for a specific population, with payments made at as large a scale as is practical. Providers and commissioners would need to agree the payment for each outcome and ensure there is appropriate outcomes data available on which payments can be informed. Payments could be higher for better outcomes at an earlier stage in pathways, incentivising providers to prevent worsening ill health.
As with QOF, there will be an administrative burden of implementation, from monitoring outcomes data to making associated payments, although this should be minimal by comparison to the potential benefits. However, the potential to make significant progress on their integrated care strategies will be a powerful incentive for ICSs. The complexity of creating and implementing and outcomes-based fee model will likely be a significant practical challenge.
A similar approach has been deployed in North Central London ICS, where UCLH is a lead provider for musculoskeletal (MSK) services across the London Borough of Camden, that is at place-level within the system footprint (please see case study below). This approach could also be taken for diabetes care, making payments based on NHS RightCare’s seven outcome targets in its model pathway. [104] We have heard most interest from ICS leaders in taking such an approach to care pathways for frail and elderly patients to help reduce secondary care admissions.
While place may be an appropriate level for commissioning such an approach and encouraging integration, the learning from the Camden MSK model is that the initial set-up time for the current model was disproportionate to the expected benefit, although this may be mitigated as best practice models are established and can be more easily replicated and rolled out. If upscaled across several different therapy areas, with different ICSs agreeing different outcomes and payments within their footprints and existing payment mechanisms remaining in place elsewhere, this approach does risk adding complexity and a creating a fragmented payment system, which could add cost and dilute incentives. It will also be important for ICSs to be able to exit the costs associated with ‘old’ care pathways/models of care. The time taken to undertake consultation and extensive scrutiny can render beneficial changes uneconomic due to the burdensome regulatory processes, but can reap rewards when agreed.
While this approach has clear benefits and may be preferable to an outcome-based payment for community care approach, further work is required to develop the proposal in sufficient detail for it to be implemented. In 2024/25, the NHS Confederation will seek to develop an outcomes-based and lead provider pilot programme, in collaboration with local leaders, which could be trialled across willing ICSs in either 2024/25 or 2025/26 to inform longer-term NHS payment policy. This will set out in further detailed proposals for such a model, including metrics for outcomes, how much is paid for delivering those metrics, the balance between fixed and variable costs and the potential benefits, risks and mitigations, with a particular focus on admissions avoidance in elderly and frailty care pathways.
Case study: Camden MSK service – outcome-based payments and a lead provider model
The musculoskeletal (MSK) service for patients in the borough of Camden was separately commissioned by the CCG to go live in 2017/18. The model was one of UCLH being a ‘lead provider’ for all MSK services, including community physiotherapy and acute pathway activity not just in UCLH but across other trusts. The service was commissioned under block population-based funding in the region of £15 million per year, with volume risk passing to UCLH and its partners, and with around 10 per cent of the contract value being tied to outcomes being achieved each year. The service also included a private sector provider of community physiotherapy.
Overall the service has been a success, delivering good outcomes and reducing the demand for acute intervention for MSK conditions. Spend on acute activity (adjusted for inflation) has reduced by 15.5 per cent, rising to 27 per cent when compared against a counterfactual of 2 per cent per annum growth that might otherwise have been expected based upon general acute growth.
However, there have also been some significant challenges:
- The amount of time and effort to set the contract up and manage subcontractors is very significantly disproportionate to the value of the contract (which represents around 1 per cent of UCLH’s turnover).
- The agreement of outcomes measures, and the measurement against them, proved to be complex and the tying of financial payments/penalties to achievement or otherwise of outcome metrics meant that these were harder to agree.
- The ‘value for money’ that the service has delivered is still often quantified by the ICB in terms of the amount of PbR-type activity undertaken (which is less, a success of the model).
- The interaction between this contract and the ever-changing way in which elective activity is funded post pandemic has been challenging to understand (although not material given that activity levels are broadly level from year to year so there is no material double or non-payment of elective activity).
- The need to procure the service separately adds further to the complexity, particular given the nature of the service which includes private sector providers. Each time the service comes up for renewal there is further uncertainty for staff running the service, which is unhelpful.
Overall it took several years for the service to mature, to thrive and to have the right contracts in place. While it has been a strong success in many ways, this was at a cost in terms of management and contracting capacity. From an ICB perspective the block contract is simple, but the commissioning responsibility and workload is shifted to the lead provider and has probably increased in totality rather than reduced.
In future: Capitated risk-based payments
In the longer term, we should look further ahead of these two models for a more comprehensive payment system to underpin ICS developments. Looking abroad, the OptiMedis approach in Germany, ChenMed in the USA and Kaiser Permante in the US point to a way forward, achieving better health outcomes for less money (see case studies below). The crucial learning from these systems is not how money is raised – the debate between public and private insurance funding – but how it is spent through different payment mechanisms and the incentives these create. Elements of this approach have already been tested in the UK, with the deployment of capitated outcome-based and incentivised contracts (COBICs) in Milton Keynes and elsewhere (see case study below).
This model would involve the introduction of multi-year, capitated payments across systems, with shared savings contracts between ICBs and multiple providers, as a more radical, longer-term approach. These would be risk weighted, reflecting higher healthcare need and likely expense from factors such as age, deprivation and rurality (geographic dispersal) of the population. This approach would seek to incentivise earlier-stage interventions and integrated working by emulating the international best practice approaches, tailored to an ICS environment.
Significant further work is required to consider the different ways such an approach could be applied more broadly to the English context. One such way may be for ICBs and vertical provider collaboratives to agree expected costs for providing secondary care – any differences with actual healthcare costs (for instance, from using non-secondary care interventions) would be considered savings and split between providers and ICBs through a shared savings contract. Minimum quality standards (aligning with national clinical standards) would be set, with deductions in payments for activity falling below the standard. This could include elements of outcome-based payment, building on the second model. Like the previous model, this would allow providers to retain savings from allocative efficiency, although allowing commissioners to keep some of the revenue. It would also feature some payment relating to outcomes. Compared to GP capitation payments, it would need to cover multiple care settings and ensure gain-share between providers and commissioners, while avoiding the complexity of payments currently associated with the mix and multitude of capitation, QOF and IIF payments for general practice.
This approach would require significant improvements in how we collate, integrate and monitor data. It would require data on expected and actual costs to be calculated and observed so appropriate shared savings contracts between providers and commissioners, and data on standards to be collected and monitored, with an appropriate discount for missing standards to be agreed. Multi-year contracts would enable systems to invest in more services with a return on investment that spans more than one financial year, but by its nature it would take longer for this approach to help achieve financial balance, a particular challenge when system financial plans are under pressure. Implementing this approach across a wide range of therapy areas would require more time to agree appropriate outcomes metrics and the tools and technology to monitor activity and outcomes. Additionally, determining and allocating gain-share is complex.
We propose that further policy development is undertaken to consider how a capitated risk-based payments could be applied to the English context and ICSs, with a view to local experimentation in 2025 and into the future.
Case study: Capitated outcome-based and incentivised contracts (COBICs) xi
In 2011, commissioners in Milton Keynes took a new approach to commissioning their substance misuse and sexual health services to improve the quality of services, their value for money and patient outcomes. In order to align financial incentives with system goals the contracts were multi-year (rather than annual) and comprised of capitation and outcome-based payments. The outcome indicators were co-produced with service users and provide additional income for providers for improved performance.
Implementing these outcome-based and incentivised contracts (also known as COBIC) led to services which were better coordinated, delivered at lower costs and produced better outcomes. They also created a more patient-centre service through the use of patient-defined outcomes and led to changes to the collection and monitoring of data.
Collaboration between different providers and partners is key to ensuring patient-led outcomes are achieved, which this model sought to incentivise. The multi-year capitated element also incentivised providers to improve population health and invest in prevention.